Fill in a Valid Cna Shower Sheets Template
Common mistakes
-
Neglecting to perform a thorough visual assessment: Some individuals may rush through the skin assessment, leading to missed abnormalities.
-
Failing to report abnormalities promptly: It is crucial to inform the charge nurse immediately about any unusual findings. Delays can impact resident care.
-
Inaccurate documentation: Omitting details or mislabeling the location and description of skin issues can create confusion and hinder proper treatment.
-
Ignoring the body chart: Not using the provided body chart to mark abnormalities can result in a lack of clarity regarding the resident's condition.
-
Overlooking toenail care: Forgetting to check if the resident needs toenail trimming can lead to discomfort or health issues.
-
Not obtaining necessary signatures: The form must be signed by both the CNA and the charge nurse. Missing signatures can delay follow-up actions.
-
Failing to forward information to the Director of Nursing (DON): If abnormalities are not communicated to the DON, appropriate interventions may not be implemented.
Learn More on This Form
-
What is the purpose of the CNA Shower Sheets form?
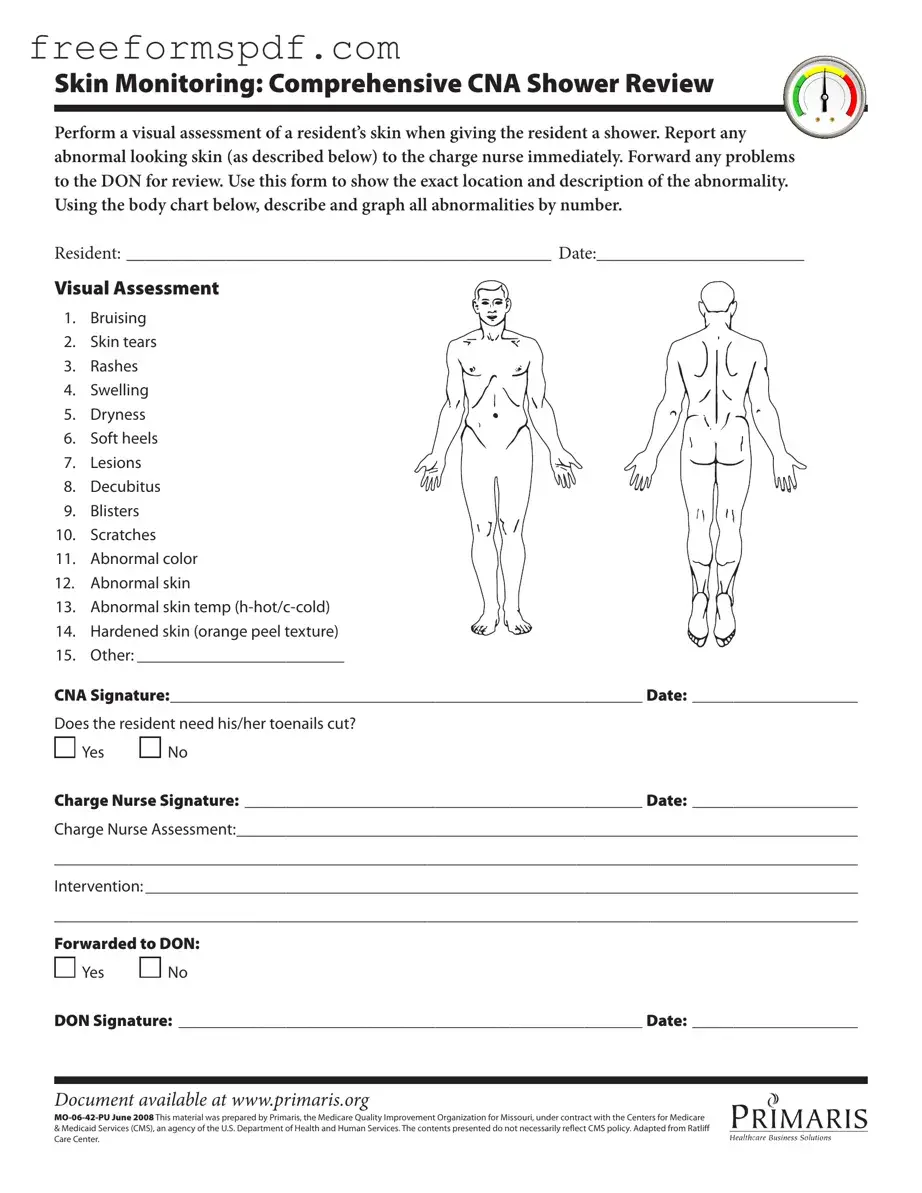
The CNA Shower Sheets form is designed to facilitate the visual assessment of a resident's skin during showering. It helps in documenting any abnormalities such as bruising, rashes, or lesions, ensuring that these issues are reported to the charge nurse promptly for further evaluation.
-
Who is responsible for completing the CNA Shower Sheets form?
The Certified Nursing Assistant (CNA) is responsible for completing the form. They perform the visual assessment of the resident's skin and document any findings, ensuring that any concerns are communicated to the charge nurse.
-
What types of skin abnormalities should be reported?
Common abnormalities to look for include:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus (pressure sores)
- Blisters
- Scratches
- Abnormal color
- Abnormal skin temperature
- Hardened skin with an orange peel texture
- Any other issues that may arise
-
How should abnormalities be documented on the form?
Abnormalities should be documented by describing their exact location and characteristics. The form includes a body chart where the CNA can graphically indicate the areas affected by numbering the abnormalities.
-
What should be done if an abnormality is found?
If an abnormality is identified, it must be reported to the charge nurse immediately. The charge nurse will then assess the situation and determine the appropriate intervention. Any significant findings should also be forwarded to the Director of Nursing (DON) for further review.
-
Is there a section for toenail care on the form?
Yes, the form includes a question regarding whether the resident needs their toenails cut. The CNA should answer "Yes" or "No" based on their assessment.
-
What happens after the charge nurse reviews the form?
After the charge nurse reviews the form, they will document their assessment and any interventions taken. This ensures a clear record of the resident's condition and the actions taken in response to any identified issues.
-
Who signs the form after the assessment is completed?
The form requires signatures from both the CNA who conducted the assessment and the charge nurse who reviewed it. Additionally, if the findings are forwarded to the DON, their signature is also required.
-
Where can the CNA Shower Sheets form be accessed?
The form is available online at www.primaris.org. This allows for easy access and ensures that the most current version is used.
-
Is the information in the CNA Shower Sheets form confidential?
Yes, the information documented in the form is considered confidential and should be handled in accordance with privacy regulations. It is important to ensure that resident information is protected and only shared with authorized personnel.
Misconceptions
Misconceptions about the CNA Shower Sheets form can lead to misunderstandings regarding its purpose and use. Here are seven common misconceptions:
- The form is only for reporting serious skin issues. Many believe that the CNA Shower Sheets form is only necessary for severe problems. In reality, it is essential for documenting all skin assessments, even minor issues.
- Only the charge nurse can fill out the form. Some think that only the charge nurse is authorized to complete the form. However, certified nursing assistants (CNAs) are responsible for the initial assessment and documentation.
- The form is optional. There is a misconception that using the form is a choice. In fact, it is a vital part of the care process and helps ensure proper monitoring of residents’ skin health.
- All skin abnormalities require immediate treatment. Some may assume that every abnormal finding must be treated at once. While prompt reporting is necessary, the charge nurse will determine the appropriate intervention.
- The body chart is only for visual reference. Many people think the body chart is just a visual aid. In truth, it is crucial for accurately documenting the location of skin abnormalities.
- The form is only relevant for elderly residents. There is a belief that the form applies solely to older adults. However, it is important for all residents, regardless of age, to be assessed for skin conditions.
- Documentation is not necessary if no issues are found. Some may think that if no abnormalities are noted, the form does not need to be completed. However, documentation of the assessment is essential, even when skin appears healthy.
Understanding these misconceptions can improve the quality of care provided to residents and ensure that all skin assessments are properly documented.
Browse More Forms
Reg 262 Dmv - Maintain a copy of this form in your vehicle for reference during transactions.
When engaging in the sale of a vehicle, it's essential to have a Motor Vehicle Bill of Sale, as this document serves as a crucial record of the transaction, ensuring a clear understanding between the buyer and seller. To assist you in this process, you can access a helpful resource at https://newyorkform.com/free-motor-vehicle-bill-of-sale-template, which provides a free template to simplify the creation of this important document.
Blank Bill of Lading - It is vital for businesses to understand their rights and responsibilities outlined in the bill.
Hazmat Bol - Packages must be marked clearly as containing hazardous materials.